
Syringomyelia (SM) MRI Screening Protocol

The British Veterinary Association (BVA) and the UK's Kennel Club (KC) issued in March 2012 a new syringomyelia MRI screening protocol, for complying with the BVA/KC's set of Chiari-like malformation and syringomyelia (CM/SM) breeding guidelines, with the aim of removing from breeding programs, cavalier King Charles spaniels with early-onset SM, and thereby reducing or even eliminating the incidence of CM/SM in future generations of cavaliers.
The MRI screening protocol is available in a downloadable pdf version at Dr. Clare Rusbridge's website by clicking here. A current list of MRI-scanned cavaliers is available by clicking here.
This MRI screening protocol should be followed everywhere in the world, to assure uniform application to the CM/SM Grading Scales, which are a set of uniform standards which any veterinary neurologist or other veterinary specialist should use to grade any cavalier's MRI scan.
RETURN TO TOP
Current Research
November 2014:
Belgian researchers find no significant difference
between CT scans and MRI scans detecting Chiari-like malformation in
cavaliers.
 In
a November 2014 study
of 15 cavalier King Charles spaniels
by a team of Belgian researchers, they compared computed tomography (CT)
scans with MRI scans and analyzing them statistically, they found "no
significant difference between the different observers and techniques
for the detection of CH [cerebellar herniation] and measurement of CHL
[cerebellar herniation length]." However, they found "Overall, the CHL
was longer on the CT images." They concluded:
In
a November 2014 study
of 15 cavalier King Charles spaniels
by a team of Belgian researchers, they compared computed tomography (CT)
scans with MRI scans and analyzing them statistically, they found "no
significant difference between the different observers and techniques
for the detection of CH [cerebellar herniation] and measurement of CHL
[cerebellar herniation length]." However, they found "Overall, the CHL
was longer on the CT images." They concluded:
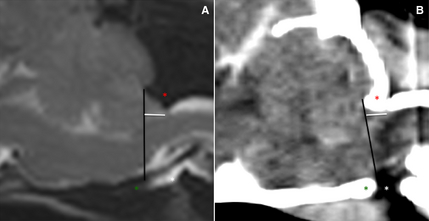
"Both techniques are useful for detecting CH and measuring CHL. Because CHL does not have a known direct impact on the clinical presentation of CM, CT can be used as a diagnostic tool in a routine clinical practice for CM in CKCS when MRI is not available. We emphasize that MRI is the standard screening technique in CKCS for breeding purposes to detect the presence of CM and SM and, at the current time, CT cannot replace MRI."
The two images above are (A) an MRI midsagittal T2WSE image and (B) a postcontrast CT image (soft tissue window) of the brain of the same CKCS. The supraoccipital bone (red asterisk), basioccipital bone (green asterisk) and occipitoatlantoaxial joint is visible (white asterisk). The foramen magnum limit is set (black line) from the rostrodorsal aspect of the supraoccipital bone to the most caudal aspect of the basioccipital bone. The cerebellar herniation length (mm, white line) is measured caudal from the foramen magnum. See also, this March 2014 item below.
July 2014: UK's Dr. Jacques Penderis finds MRI noise results in some hearing loss in dogs. In a study of 36 dogs, a Univerisity of Glasgow team lead by Dr. Jacques Penderis found that exposure to noise during MRI scans results in significant reductions in cochlear function at five of fourteen frequencies. It is not known whether the hearing loss is reversible or permanent. See more details in the November 2013 entry below.
March
2014:
Belgium researchers find computed tomography (CT) can be used to
diagnose
 Chiari-like
malformation in CKCSs. In a
2013 study of nine cavaliers with neurological disorders, a team of
Ghent University (Belgium) veterinary radiologists compared the dogs' MRIs
and computed tomographs (CT) and concluded:
Chiari-like
malformation in CKCSs. In a
2013 study of nine cavaliers with neurological disorders, a team of
Ghent University (Belgium) veterinary radiologists compared the dogs' MRIs
and computed tomographs (CT) and concluded:
"The statistical analysis suggested that both techniques are useful for detecting CH [cerebellar herniation]. However because the bias was significantly different from zero, one of the methods consistently led to the determination of longer or shorter HL [cerebellar herniation length] than the other method. For most comparisons, the HL was on average longer on CT. MRI provides greater soft tissue detail with no beam-hardening artifacts, which may improve the delineation of the cerebellum. Because HL does affect a diagnosis of CM, so CT can be used as a primary diagnostic tool for diagnosing CM in CKSs when MRI is not available."
November 2013: Univ. of Glasgow thesis reports MRI noise causes hearing loss and reduced cochlear function in dogs. In a 2013 Master of Science (Research) thesis at the University of Glasgow, Rebecca Elisabeth Venn reports that all of 36 dogs (including four cavalier King Charles spaniels) which underwent MRI scans, experienced reduced cochlear function and more than half of the 36 dogs had hearing loss using Distortion Product Otoacoustic Emissions (DPOAE) testing. Ms. Venn noted that the post-MRI testing was not repeated weeks after the MRIs, so it is not known if the hearing loss was temporary or permanent. She also noted that evidence from human MRI noise exposure suggests that the hearing loss is temporary. She recommends that "all dogs having MRI studies performed should have ear protection as a standard precautionary measure." See also the July 2014 entry above.
November 2013: UK researcher finds MuttMuff "ear defenders" suitable for dogs during MRI scans. In a November 2013 study exclusively of cavalier King Charles spaniels, Professor Martin Baker of the University of Liverpool reported that MuttMuff "ear defenders' -- an ear muff device -- were safe to use during MRI scans at 1 T. He stated that, "For brain scans the ear defenders assist in the immobilisation of the dog's head within the coil."
August 2011: Head position affects extent of cerebellar herniation in MRI scans. UK researchers examining 14 CKCS MRI scans (7 with CM/SM and 7 with just CM) comparing scans in both extended and flexed head positions. In their report, they have found the degree of cerebellar herniation was significantly worse in dogs with a flexed compared to an extended head position. When cerebrospinal fluid (CSF) space between the cerebellum and brainstem was compared in CKCS with and without SM, there was a significant increase in CSF space in CKCS with CM alone compared to those with CM/SM when head position was flexed. Based upon their findings, they state that it may be appropriate to position patients in a more flexed head position for optimal imaging in order to identify morphologic changes more accurately. They stated that this is important to consider for imaging CKCS with CM especially when studying the pathogenesis of CM/SM.
The researchers also found:
"When CSF space between the cerebellum and brainstem was compared in CKCS with and without SM, there was a significant increase in CSF space in CKCS with CM alone compared to those with CM/SM when head position was flexed. In their cine MR imaging study of CSF flow dynamics in CKCS with CM or CM/SM, Cerda-Gonzalez and others (2009a) found that turbulent CSF flow and jets are associated with SM presence and severity and CSF flow velocity at C2/3 is inversely related to the presence of SM. The reduced CSF space in CM/SM dogs reported in this study could explain this jet like CSF flow in dogs with CM/SM compared to those with CM alone."
This could mean that the severity of CM/SM, or even the presence or future presence of SM, could be predicted based upon the measure of cerebrospinal fluid space between the cerebellum and the brainstem. If so, this could go a long way to distinguishing whether a CM-only cavalier is either likely or unlikely to develop SM in the future. This distinction could be a way to fine-tune a breeding protocol, considering that we now know that over half of cavaliers with SM develop it after their 3rd birthday. If we could reliably count on this measurement of CSF space to tell us if a young dog will, or will not, develop SM in the future, then we could more reliably select SM-free breeding stock at a younger age than the present 2.5 years and the 3+ years the researchers may recommend in the future.
RETURN TO TOP
Related Links
RETURN TO TOP
Veterinary Resources
Neurological signs and results of magnetic resonance imaging in 40 cavalier King Charles spaniels with Chiari type 1-like malformations. Lu D, Lamb CR, Pfeiffer DU, Targett MP. Vet Rec. Aug 2003;153(9):260-3.
The Use of Ultrasonography to Diagnose “Caudal Occipital Malformation Syndrome” in Dogs – a Prospective Study in 12 Dogs. B Levitin, JJ McDonnell, D Faissler, AS Tidwell. J Vet Intern Med; May/June 2005;19(3) (ACVIM 23rd Ann. Vet. Med. Forum Abstract Program: Abstract 209).
Brain Stem Auditory Evoked Response (BAER) Testing in Cavalier King Charles Spaniels with Caudal Occipital Malformation Syndrome. CW Dewey, KS Bailey, G Barone, J Stefanacci. J Vet Intern Med; May/June 2006;20(3) (ACVIM 24th Ann. Vet. Med. Forum Abstract Program: Abstract 270).
Syringomyelia in cavalier King Charles spaniels: the relationship between syrinx dimensions and pain. C Rusbridge, H Carruthers. M-P Dubé, M Holmes, N D Jeffery. J Small Anim. Pract. 2007 Aug;48(8):432-6. Quote: "Objectives: This study was designed to test the hypothesis that pain associated with syringomyelia in dogs is dependent upon size and involvement of the dorsal part of the spinal cord. Methods: Masked observers determined syrinx dimensions and precise location within the spinal cord on magnetic resonance images of 55 cavalier King Charles spaniels with syringomyelia. After removal of masking, syrinx size and location were compared between the cohorts of dogs that exhibited pain with those that did not. Results: Maximum syrinx width was the strongest predictor of pain, scratching behaviour and scoliosis in dogs with syringomyelia. Both pain and syrinx size were positively correlated with syrinxes located in the dorsal half of the spinal cord. Clinical Significance: Large syrinxes associated with damage to the dorsal part of the spinal cord are associated with persistent pain suggesting that the pain behaviour expressed by this group of patients is likely to be 'neuropathic pain', resulting from disordered neural processing in the damaged dorsal horn. As such it is likely that conventional analgesic medication may be ineffective."
Magnetic resonance imaging - unravelling the mystery. J. Fraser McConnell. J Small Anim. Pract. 2007 Aug;48(8): 421-422. Quote: "With evidence based medicine in vogue the study by Claire Rusbridge and colleagues (Rusbridge and others 2007) is to be congratulated and is of particular value as it contains a cohort of dogs with no clinical signs. Obtaining MR images of neurologically normal animals can be difficult as it is often not possible to justify anaesthesia in such animals. The use of MRI screening prior to breeding gives valuable information from a group of clinically normal animals. ... Reliance on statistical analyses alone can be misleading when it comes to determining the significance of MRI changes for an individual animal. While the diagnosis of syringohydromyelia in cavalier King Charles spaniels is straightforward with MRI, the problem is one of interpreting what the changes will mean for an individual. It has long been recognised that there is a poor correlation between severity of MRI abnormalities and whether the dog will show clinical signs with syringomyelia. This was shown by Lu and others (2003) who found no correlation between the severity of the syrinx and presence of neurological signs relating to the spine; some dogs with marked syringomyelia having no spinal signs (Lu and others 2003). The study by Rusbridge and colleagues in this issue reports different results and found, not surprisingly, that the larger the syrinx the more likely the individual will show clinical signs. While the study suggests that assessing syrinx size based on transverse plane images may be a more useful method than length of syrinx this does not give all the answers to the problem of interpretation. The data shows that while there is a good correlation between size of syrinx and pain there is an almost complete overlap of the range of syrinx size between the two groups. The significance of this is that it is still not possible to state with certainty, based on the MRI findings, whether a dog will develop clinical signs. It is likely that functional imaging such as CSF flow studies will be required to unpick the complexity of syringomyelia in cavalier King Charles spaniels. Similar findings have been reported in other areas of neuroimaging such as degenerative lumbosacral stenosis and intervertebral disk disease (Penning and others 2006, Mayhew and others 2002, Suwankong and others 2006) It is clear that with all the advances in imaging techniques there are still no easy answers. Imaging findings must be interpreted in light of the clinical findings and support rather than replace the neurologist or neuropathologist!"
Radiographic morphology of the cranial portion of the cervical vertebral column in Cavalier King Charles Spaniels and its relationship to syringomyelia. Stalin CE, Rusbridge C, Granger N, Jeffery ND. Am J Vet Res. 2008 Jan;69(1): 89-93. Quote: "Results suggested that radiographic morphology of the atlantoaxial region in CKCSs differs from morphology of that region in dogs of other breeds, but that these differences do not account for why some CKCSs develop syringomyelia and others do not."
Use of magnetic resonance imaging for morphometric analysis of the caudal cranial fossa in Cavalier King Charles Spaniels. Carrera I, Dennis R, Mellor DJ, Penderis J, Sullivan M. Am J Vet Res; 2009 Mar;70(3):340-5. Quote: "Objective-To perform morphometric analysis of the caudal cranial fossa in Cavalier King Charles Spaniels (CKCSs), to assess the relationship between caudal fossa dimensions and the frequency of magnetic resonance imaging (MRI) features of occipital abnormalities in CKCSs (with and without syringomyelia), and to compare caudal cranial fossa measurements in CKCSs with measurements of 2 groups of mesaticephalic dogs. Animals-70 CKCSs and 80 mesaticephalic (control) dogs. Procedures-Dogs were placed into 4 groups as follows: Labrador Retrievers (n = 40), spaniel-type dogs (40; English Springer Spaniels and Cocker Spaniels), CKCSs with syringomyelia (55), and CKCSs without syringomyelia (15). Multiple morphometric measurements (linear, angular, and area) were obtained from cranial midsagittalT2-weighted magnetic resonance images including the brain and cervical portion of the spinal cord. Several specific MRI findings were also recorded for CKCSs that appeared to affect the occipital bone and cervicomedullary junction. Results-No significant difference was identified among breeds in control groups and between sexes in any of the groups for all morphometric measurements. Significant differences were identified in CKCSs, compared with mesaticephalic dogs, in the area of the caudal cranial fossa and for several linear measurements that reflected the length of the ventral aspect of the occipital bone. These differences were greater in CKCSs with syringomyelia. All CKCSs had abnormalities in occipital bone shape. Conclusions and Clinical Relevance-CKCSs had a shallower caudal cranial fossa and abnormalities of the occipital bone, compared with those of mesaticephalic dogs. These changes were more severe in CKCSs with syringomyelia."
Growth of Clinical Veterinary Magnetic Resonance Imaging. Patrick R. Gavin. Vet.Rad. & Ultra.; Mar/Apr 2011; 52(s1):52-54. "In the spine, MR imaging reveals conditions which were previously difficult to diagnose ante-mortem, and may facilitate study of their pathophysiology. Examples include syringohydromyelia associated with Chiari-like malformation in the Cavalier King Charles spaniel... ."
Correlating Magnetic Resonance Findings with Neuropathology and Clinical Signs in Dogs and Cats. Charles H. Vite, Johnny R. Cross. Vet.Rad. & Ultra. Mar/Apr 2011; 52(1),Supp. 1:S23–S31.
Influence of head positioning on the assessment of Chiari-like malformation in Cavalier King Charles spaniels. J. J. Upchurch, I. M. McGonnell, C. J. Driver, L. Butler, H. A. Volk. Vet Rec Aug2011; doi:10.1136/vr.d4395. Quote: "Chiari-like malformation (CM) is almost omnipresent in the Cavalier King Charles spaniels (CKCS), often leading to syringomyelia (SM). Morphometric studies have produced variable results concerning relationship between the brain parenchyma within the caudal cranial fossa (CCF) and SM. The present study assesses the effect of head position, one potential confounder. Magnetic resonance images of CKCS with CM were reviewed in extended and flexed head positions. ... Fourteen CKCS were included into the study, seven dogs with CM and seven with CM/SM. ... The degree of cerebellar herniation was significantly worse in dogs with a flexed compared to an extended head position. ... Cerebellar herniation did not differ significantly between CKCS with and without SM in the extended head position. However, in the flexed head position the cerebellum herniated more caudally in CKCS with CM/SM compared to CKCS with CM alone. This highlights that the non-flexed head position may underestimate the true extent of cerebellar herniation and could explain why previous studies have missed an association with SM. ... It is well documented that flexing the head opens the CSF space of the cisterna magna and this could explain the morphometric measurements. The brainstem reduces in size to accommodate this increase in CSF space. ... When CSF space between the cerebellum and brainstem was compared in CKCS with and without SM, there was a significant increase in CSF space in CKCS with CM alone compared to those with CM/SM when head position was flexed. ... The reduced CSF space in CM/SM dogs reported in this study could explain this jet like CSF flow in dogs with CM/SM compared to those with CM alone. ... Furthermore, there is an association between head position and level of foramen magnum overcrowding. Based on these findings it may be appropriate to position patients in a more flexed head position for optimal imaging in order to identify morphologic changes more accurately. This is important to consider for imaging CKCS with CM especially when studying the pathogenesis of CM/SM. It should also be considered when taking a cisternal CSF sample as the spinal needle might be traumatic to the herniated cerebellum."
Distribution of syringomyelia along the entire spinal cord in clinically affected Cavalier King Charles Spaniels. Shenja Loderstedt, Livia Benigni, Kate Chandler, Jacqueline M. Cardwell, Clare Rusbridge, Christopher R. Lamb, Holger A. Volk. Vet J Dec 2011;190:359–363. Quote: "The objective of the present study was to define the anatomic distribution of SM in CKCS clinically affected by CM/SM. Our hypotheses were that in dogs with SM, (1)SM is present at multiple locations throughout the whole spinal cord; (2) the prevalence of SM is greatest in the cervical spine versus other regions; (3) the presence of SM in the cervical spinal cord is associated with the presence of SM in further caudal spinal cord regions; (4) the maximal syrinx size in each patient is in the cervical spine, and (5) there is a positive association between patient age and total syrinx size. ... 49 dogs were included in the present study. The median age of the dogs included in the study was 5 years (1.2–10.8 years). CM was present in all patients. ... All dogs in the present study were clinically affected. ... However, in our study SM was absent in 25% of dogs with clinical signs. ... There was no evidence of SM on MRI in 12/49 (25%) dogs. In all dogs with MRI evidence of SM (37/49; 75%), SM was present within the C1–C4 region (Figs. 2 and 3). Of those dogs with SM within C1–C4 region, 76% (28/37) also had SM within the C5–T1 and/ or T2–L2 regions, but only 49% (18/37) had SM within the L3–L7 region. ... The results of our investigation show that imaging only the cervical spine in clinically affected CKCSs is likely to underestimate the total syrinx size and the anatomical distribution of SM. The presence of cervical SM in all dogs with MRI evidence of SM could however justify the restricted imaging under screening purposes. ... The results of our study showed syrinx formation in all regions of the spinal cord with no significant differences of Sx between the cervical, cervicothoracic and thoracolumbar regions, but significantly smaller Sx in the caudolumbar spinal region. ... In our study Smax was most often seen within the C1–C4 region and, interestingly, also over T2–L2 vertebral bodies. ... We found that the severity of SM was positively correlated with patient age. This is consistent with previous studies indicating that CKCS with SM were significantly older than dogs without SM (Couturier et al., 2008). It seems likely therefore, that SM is a progressive disease in dogs. ... Conclusions: There is a very high potential for CKCS with clinical signs of CM/SM to develop SM in more than one spinal cord region. Diagnostic imaging limited to the cervical spine in clinically affected CKCS is likely to underestimate the degree and severity of SM. It can be hypothesised that SM has a progressive nature in CKCS, which requires further characterisation."
MRI acoustic noise can harm experimental and companion animals. Amanda M. Lauer, AbdEl-Monem M. El-Sharkawy, Dara L. Kraitchman, William A. Edelstein. J. Magnetic Resonance Imaging. 2012;36:743-747. Quote: "Purpose: To assess possible damage to the hearing of experimental and companion animal subjects of magnetic resonance imaging (MRI) scans. Materials and Methods: Using animal hearing threshold data and sound level measurements from typical MRI pulse sequences, we estimated ‘‘equivalent loudness’’ experienced by several experimental and companion animals commonly subjects of MRI scans. We compared the equivalent loudness and exam duration to safe noise standards set by the National Institute for Occupational Safety and Health (NIOSH). Results: Monkeys, dogs, cats, pigs, and rabbits are frequently exposed to equivalent loudness levels during MRI scans beyond what is considered safe for human exposure. The sensitive frequency ranges for rats and mice are shifted substantially upward and their equivalent loudness levels fall within the NIOSH safe zone. Conclusion: MRI exposes many animals to levels of noise and duration that would exceed NIOSH human exposure limits. Researchers and veterinarians should use hearing protection for animals during MRI scans. Experimental research animals used in MRI studies are frequently kept and reimaged, and hearing loss could result in changed behavior. Damage to companion animals’ hearing could make them less sensitive to commands and generally worsen interactions with family members. Much quieter MRI scanners would help decrease stress and potential harm to scanned animals, normalize physiology during MRI, and enable MRI of awake animals."
Magnetic Resonance Imaging (MRI) Spinal Cord and Canal Measurements in Normal Dogs. S. Hecht, M. M. Huerta, R. B. Reed. Anatomia Histologia Embryologia. March 2013. Quote: "The goal of this study was to establish Magnetic resonance imaging (MRI) reference ranges for spinal measurements in normal dogs. Forty dogs (1–10 kg, 11–20 kg, 21–30 kg, > 30 kg; 10 dogs per category) underwent spinal MRI. Measurements were performed on sagittal T2-W images at the level of the 4th thoracic vertebra (T4), the 9th thoracic vertebra (T9) and the 3rd lumbar vertebra (L3). Spinal canal diameter (mm) ranged from 6.07 ± 0.63 (1–10 kg) to 8.27 ± 1.15 (> 30 kg) at the level of T4; 6.55 ± 0.61 (1–10 kg) to 9.04 ± 1.26 (> 30 kg) at the level of T9; and 6.80 (6.47–7.00; 1–10 kg) to 9.00 (7.90–9.73; > 30 kg) at the level of L3. There were significant differences (P < 0.05) in spinal canal diameter between groups. Mean spinal cord diameter (mm) ranged from 4.46 ± 0.51 (11–20 kg) to 4.70 ± 0.35 (1–10 kg) at the level of T4; 4.41 ± 0.50 (> 30 kg) to 4.85 ± 0.57 (1–10 kg) at the level of T9; and 4.52 ± 0.51 (> 30 kg) to 5.14 ± 0.68 (1–10 kg) at the level of L3. There were no significant differences in spinal cord diameter between groups. Spinal cord-to-spinal canal ratio varied significantly, ranging from 0.51 ± 0.08 (> 30 kg at L3) to 0.78 (0.69–0.80; 1–10 kg at T4) (P < 0.05). These findings are important when using MRI to evaluate patients with suspected diffuse spinal cord disease."
The Effects of Magnetic Resonance Imaging Noise on Cochlear Function in Dogs. Chapter 2 of "Effects of acute and chronic noise exposure on cochlear function and hearing in dogs." Rebecca Elisabeth Venn. MSc(R) thesis pp 21-42, University of Glasgow. 2013. Quote: "In specialised veterinary hospitals, Magnetic Resonance Imaging (MRI) scanners are used daily in diagnostics of dogs. MRI scanners omit high levels of acoustic noise, which is known to be damaging to the hearing of human patients without effective ear protection. However, the effects of the MRI noise levels on the cochlear function and hearing of dogs is often overlooked and in many clinics, dogs are not provided with ear protection for the duration of their scan. The aim of this study was to assess the effects of MRI acoustic noise on the cochlear function of dogs, by Distortion Product Otoacoustic Emissions (DPOAE) testing dogs immediately before and after they underwent an MRI scan. ... Thirty-six dogs were included in the MRI group (mean age 3.9 years, median age 3 years, range 6 months to 10 years; mean bodyweight 16.9 kg, median bodyweight 13.8 kg, range 3.5 kg to 40.8 kg) and 17 dogs were included in the control group (mean age 6.2 years, median age 7 years, range 1 year to 12 years; mean bodyweight 25.1 kg, median bodyweight 23.6 kg, range 6.7 kg to 57.8 kg). There were 16 male dogs in the MRI group (44.4%) and 10 male dogs in the control group (58.8%). A variety of dog breeds were represented, with those represented more than once including three toy poodles, three Lhasa Apso dogs, four Labrador retrievers, two cocker spaniels, four Cavalier King Charles spaniels, two boxers and three cross-breeds in the MRI group, and two Labrador retrievers and two cross-breeds in the control group.... A group of control dogs undergoing a quiet procedure (but treated with the same range of anaesthetic drugs) were also tested. Post-MRI, the mean DPOAE of the dogs was reduced at all frequencies tested, significantly so at five (out of fourteen) frequencies, reflecting a reduction in cochlear function. Furthermore, at all frequencies tested, more than half of the ears exposed to MRI noise demonstrated a decrease in DPOAE. ... The results from this study indicate that exposure to noise during MRI in dogs results in a reduction in cochlear function, which is significant at multiple sound frequencies. ... Without repeat DPOAE testing of the dogs some weeks after their MRI, it is unknown whether this effect is temporary and reversible, or permanent. ... Evidence from human MRI noise exposure would suggest that this effect is temporary. The frequency region affected is likely influenced by the frequency of the noise spectra of the MRI. The demonstration that MRI noise results in some degree of hearing loss, albeit only assessed in the immediate post-MRI period in the present study, would suggest that all dogs having MRI studies performed should have ear protection as a standard precautionary measure."
Evaluation of MR safety of a set of canine ear defenders (MuttMuffs®) at 1
T. Martin A. Baker. Radiography. Nov. 2013;19 (4):339-342.
Quote: "Previous studies have indicated that loud noise produced during MR
scanning is hazardous for human patients. Although loud noise can also be
harmful to canine patients in MRI, ear protection is not routinely provided. The
purpose of this study was to test the safety of a set of commercially available
canine ear defenders (MuttMuffs®) during MRI scanning at 1 T. ... The dogs were
all of the same breed (Cavalier King Charles Spaniel), with
half having been provided with the ear defenders and half which had not. ... A
metal fastening ring was removed and replaced with a plastic washer prior to
testing. Torque, translation, heating and artifact production were tested. No
torque, translation, or excessive heating were detected. No artifacts were
observed. Clinical use demonstrated additional benefits of improved
immobilisation of the dog, with no effect on signal-to-noise ratio. For brain
scans the ear defenders assist in the immobilisation of the dog's head within
the coil. Results from
this study indicate that following replacement of the metal ring with one made
of plastic, these canine ear defenders are suitable for use at 1 T. The author
recommends the use of ear defenders during canine MRI scans in order to reduce
the risk of hearing damage, reduce the dose needed for anaesthetic maintenance
and reduce the need for repeated MRI sequences due to movement of the dog."
(4):339-342.
Quote: "Previous studies have indicated that loud noise produced during MR
scanning is hazardous for human patients. Although loud noise can also be
harmful to canine patients in MRI, ear protection is not routinely provided. The
purpose of this study was to test the safety of a set of commercially available
canine ear defenders (MuttMuffs®) during MRI scanning at 1 T. ... The dogs were
all of the same breed (Cavalier King Charles Spaniel), with
half having been provided with the ear defenders and half which had not. ... A
metal fastening ring was removed and replaced with a plastic washer prior to
testing. Torque, translation, heating and artifact production were tested. No
torque, translation, or excessive heating were detected. No artifacts were
observed. Clinical use demonstrated additional benefits of improved
immobilisation of the dog, with no effect on signal-to-noise ratio. For brain
scans the ear defenders assist in the immobilisation of the dog's head within
the coil. Results from
this study indicate that following replacement of the metal ring with one made
of plastic, these canine ear defenders are suitable for use at 1 T. The author
recommends the use of ear defenders during canine MRI scans in order to reduce
the risk of hearing damage, reduce the dose needed for anaesthetic maintenance
and reduce the need for repeated MRI sequences due to movement of the dog."
Comparison of MRI and CT for the detection of cerebellar (foramen magnum) herniation in Cavalier King Charles spaniels. Kromhout K., Bhatti S., Van Ham L., van Bree H., Gielen I. Ghent Univ. Academic Bibliography. 2013. Quote: "Introduction: The Cavalier King Charles spaniel (CKCS) breed exhibits a high rate of Chiari-like malformation (CM). The latter is characterised by a disproportion of volume of the cerebellum and medulla oblongata compared to that of the caudal fossa. These abnormalities are associated with displacement or herniation of the most caudal areas of the cerebellum either into or through the foramen magnum (1,2). Several articles have suggested mid-sagittal magnetic resonance imaging (MRI) as the preferred technique for visualizing the caudal fossa and diagnosing CM (1,3,4). This study compares MRI and computed tomography (CT) for the detection of cerebellar herniation (CH). Materials and Methods: Nine CKCSs were presented with a various range of neurological symptoms. MRI and CT studies of their brains and cranial cervical spines were performed as part of their clinical work-up with the dogs positioned in dorsal recumbency with the head in extended position. Using sagittal T1- and T2-weighted spin echo (T1WSE and T2WSE) MRI sequences and pre- and postcontrast CT-images, the cerebellar herniation length (HL) (= the position of the tip of the cerebellar vermis relative to the foramen magnum) was measured (mm) and assigned either a grade mild (≤ 2mm) or marked (>2mm) by 2 two observers. The results were analyzed statistically. Results: There was a perfect agreement (k=1) for both observers for the detection of mild and marked CH for both techniques. However the Bland-Altman plot analyses of the HL indicated that CT and MRI findings did not agree well. The bias was significantly different from zero when comparing the HL measurements on the CT and MRI images. The limits of agreement for all measurements found the HL differed between techniques over a range of < 1,5 mm. Discussion/ Conclusion: The statistical analysis suggested that both techniques are useful for detecting CH. However because the bias was significantly different from zero, one of the methods consistently led to the determination of longer or shorter HL than the other method. For most comparisons, the HL was on average longer on CT. MRI provides greater soft tissue detail with no beam-hardening artifacts, which may improve the delineation of the cerebellum. Because HL does affect a diagnosis of CM, so CT can be used as a primary diagnostic tool for diagnosing CM in CKCSs when MRI is not available." See also Low-Field MRI and Multislice CT for the Detection of Cerebellar (Foramen Magnum) Herniation in Cavalier King Charles Spaniels.
The effect of magnetic resonance imaging noise on cochlear function in dogs. R.E. Venn, A.R. McBrearty, D. McKeegan, J. Penderis. Vet.J. July 2014. Quote: "Noise produced by magnetic resonance imaging (MRI) scanners (which can peak at a sound pressure level of 131 dB) has been shown to cause noise-induced cochlear dysfunction in people. The aim of this study was to investigate whether noise produced during MRI had a deleterious effect on cochlear function in dogs, using distortion product otoacoustic emission (DPOAE) testing, which allows frequency specific, non-invasive assessment of cochlear function. A control group comprised dogs undergoing anaesthesia of a similar duration for quiet procedures. Thirty-six dogs (66 ears) and 17 dogs (28 ears) were included in the MRI and control groups respectively. There was a reduction in DPOAE at all frequencies tested in the MRI group; a similar effect was not evident in the control group. This reduction in the MRI group was statistically significant in five of the 14 frequencies assessed (P<0.05). Exposure to noise during MRI in dogs results in a significant reduction in cochlear function, although it is not known whether this is reversible or permanent. The frequency region affected is probably influenced by the frequency of the noise spectra of the MRI. The finding that MRI noise results in hearing loss, albeit only assessed in the immediate post-MRI period, would suggest that all dogs undergoing MRI studies should have ear protection as a standard precaution. What is not evident from the present study is the longer-term effect of excessive MRI noise on hearing and further studies are also required to assess the efficacy of ear protection to protect against the effects of MRI noise in dogs." (See also the 2013 Rebecca Elisabeth Venn master's thesis above.)
Low-Field MRI and Multislice CT for the Detection of Cerebellar (Foramen Magnum) Herniation in Cavalier King Charles Spaniels. K. Kromhout, H. van Bree, B.J.G. Broeckx, S. Bhatti, L. Van Ham, I. Polis, I. Gielen. J. Vet. Int. Med. Nov. 2014. Quote: "Background: Cavalier King Charles Spaniels (CKCS) have a high prevalence of Chiari-like malformation (CM). Herniation of the cerebellum into the foramen magnum is a key diagnostic feature for CM. Midsagittal MR images are the preferred technique for visualizing cerebellar herniation (CH). Objective: To investigate whether CT can be used to diagnose CH. Animals: Fifteen client-owned CKCS dogs referred for investigation of the brain and cranial cervical spine on MRI and CT. Methods: Two reviewers retrospectively analyzed midsagittal T1WSE and T2WSE MR images and midsagittal pre- and postcontrast 2D multiplanar reformatted CT images from each dog for the presence of CH. And, if present, the length (mm, CHL) of the herniation was measured. The results were analyzed statistically. Results: There was no significant difference between the different observers and techniques for the detection of CH and measurement of CHL. Overall, the CHL was longer on the CT images. Conclusion and Clinical Importance: Both techniques are useful for detecting CH and measuring CHL. Because CHL does not have a known direct impact on the clinical presentation of CM, CT can be used as a diagnostic tool in a routine clinical practice for CM in CKCS when MRI is not available. We emphasize that MRI is the standard screening technique in CKCS for breeding purposes to detect the presence of CM and SM and, at the current time, CT cannot replace MRI." See also, Comparison of MRI and CT for the detection of cerebellar (foramen magnum) herniation in Cavalier King Charles spaniels.
CONNECT WITH US